Diagnosing hair loss in women with afro-textured hair requires special expertise. Many hair loss conditions are possible and they tend to look similar. Central centrifugal cicatricial alopecia (CCCA) can look similar to genetic hair loss and so can some types of traction alopecia. Our program for women with afro-textured hair addresses some of the unique aspects of hair loss and hair care in black women.
Hair transplantation in CCCA
Central centrifugal cicatricial alopecia (or "CCCA" for short) is a type of scarring hair loss condition in black women. Hair loss starts in the centre of the scalp and spreads outwards over time. If treated early, the condition may be halted - at least for some women. Hair transplants are possible in CCCA once the condition becomes “quiet.” By quiet, we mean that there has been no further hair loss for a period of 1-2 years.
Are hair transplants possible for CCCA?
Surgery is sometimes an option for a group of conditions known as scarring alopecias. These conditions are frequently autoimmune in nature and have names like lichen planopilaris, frontal fibrosing alopecia, central centrifugal cicatricial alopecia.
When can a hair transplant be done in CCCA ?
A hair transplant is not possible for many patients with these conditions because the condition is "active." However, once the condition becomes "quiet" - a hair transplant can be considered.
By 'quiet', several conditions must be met. These are summarized in the CCCA Hair Transplant Criteria.
DONOVAN CCCA HAIR TRANSPLANT CANDIDACY CRITERIA
In order for patients with CCCA to be a candidate for hair transplant surgery , ALL FIVE of the following criteria must be met:
1. The PATIENT should be off medications.
Ideally the patient should be off all topical, oral and injection medications to truly know that the disease is "burned out (burnt out)". However, in some cases, it may be possible to perform a transplant in someone with CCCA who is using medications AND who meets criteria 2, 3 and 4 below. This should only be done on a case by case basis and in rare circumstances. It is a last resort in a very well-informed patient.
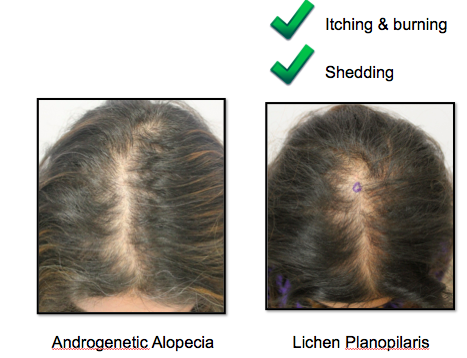
2. The PATIENT must not report symptoms related to the CCCA in the past 12 months, (and ideally 24 months) .
The patient must have no significant itching, burning or pain. One must always keep in mind that the absence of symptoms does NOT prove the disease is quiet but the presence of symptoms certainly raises suspicion the disease could be active. Even the periodic development of itching or burning from time to time could indicate the disease has triggers that cause a flare and that the patient is not a candidate for surgery. The patient who dabs a bit of clobetasol now and then on the scalp to control a bit of itching may also have disease that is not completely quiet.
3. The PHYSICIAN must make note of no clinical evidence of active CCCA in the past 12 months, (and ideally 24 months).
There must be no scalp clinical evidence of active CCCA such as hair fragility or scalp erythema. . This assessment is best done with a patient who has not washed his or her hair for 48 hours. Some scalp redness may be persistent in patients with scarring alopecia even when the disease is quiet. Therefore scalp redness alone does not necessarily equate to a concerning finding. Perifollicular redness however is more concerning for disease activity. In addition, the pull test must be completely negative for anagen hairs and less than 4 for telogen hairs. A positive pull test for anagen hairs indicates an active scarring alopecia regardless of any other criteria.
4. Both the PATIENT and PHYSICIAN must show no evidence of ongoing hair loss over the past 12 months (and ideally 24 months).
There must be no further hair loss over a period of 24 months of monitoring OFF the previous hair loss treatment medications. This general includes the patient and physician's perception that there has been no further loss as well as serial photographs every 6-12 months showing no changes.
5. The patient must have sufficient donor hair for the transplant.
Not all patients with CCCA maintain sufficient donor hair even if the disease has become quiet. But this is an important and final criteria.


![mature%20and%20balding[1].jpg](https://images.squarespace-cdn.com/content/v1/5243dccde4b08fd9e4fc92ef/1381296519700-CV7E2TO9YL5WSSBWOS9F/mature%2520and%2520balding%5B1%5D.jpg)