Side effects of Steroid Injections: What side effects do we need to counsel patients?
Before one begins steroid injections, it’s important to review possible short term and long term steroid-related side effects with the patient and get their permission (consent) to do the injections. I won’t go into all the possible side effects but the main message here is that side effects are actually not common with appropriate technique.
Short term steroid injections: What do we need to counsel patients?
The main side effects of a single session of steroid injections include:
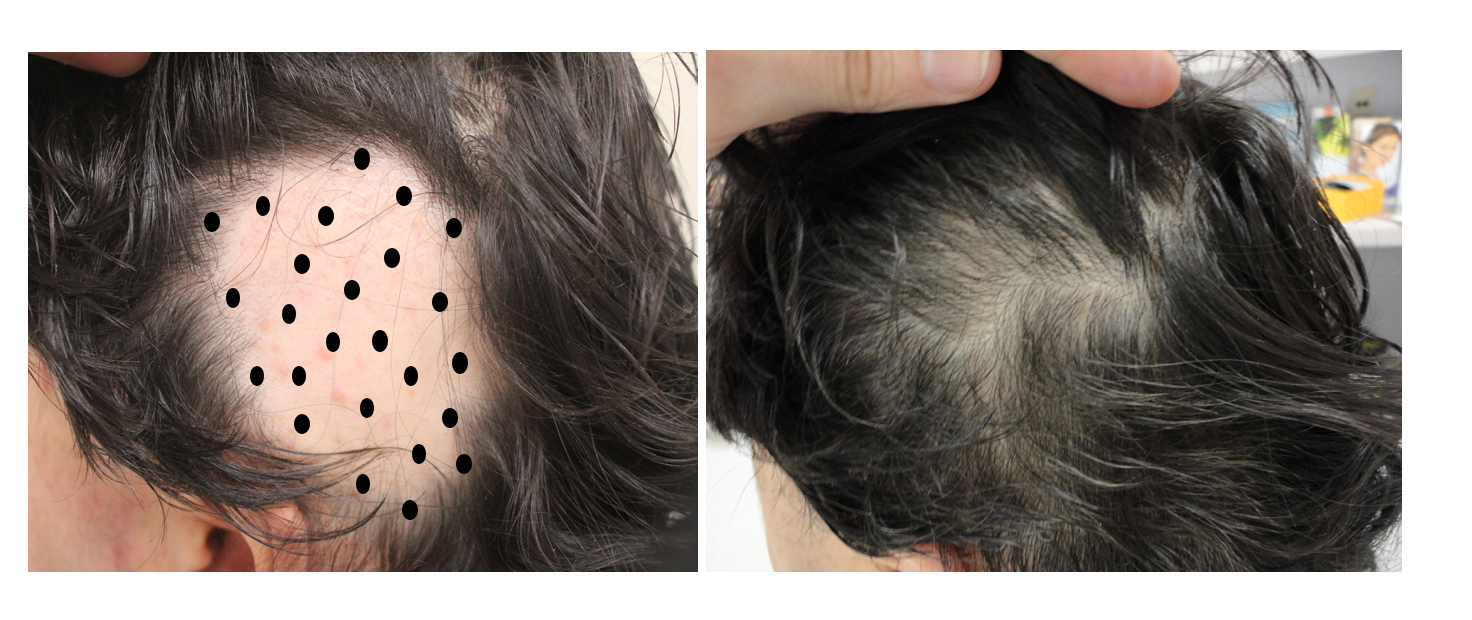
1. Minor Pain and Bleeding with injections. Steroid injections are not extremely painful but they can be uncomfortable. They are usually more uncomfortable for patients the first time they receive injections than in subsequent visits. This is likely because the effect of stress heightens pain for many patents. Many patients will say that the pain is a 3 out of 10 (with 10 being maximum). The pain is highest in the frontal hairline and especially above and around the ears compared to the middle of the scalp. The crown area is a bit more painful than the middle of the scalp. In general though pain is mild. Use of a vibration device and chatting with patients and taking many breaks during the procedure can reduce pain and discomfort a lot. Steroid injections can be performed in children over 12 using these types of basic principles. Small amounts of bleeding are possible with injections but these are easily stopped with light pressure form a gauze. Patients using blood thinners and patients who are very nervous (and have higher heart rates), may bleed a bit more - but this is seldom ever an issue that can’t be stopped with pressure from a gauze.
2. Minor soreness in the scalp after injections. In the first 24-48 hours the scalp can be a bit sore. it is usually extremely minor and relieved partially or completely with use of acetominophen or ibuprofen if necessary. Most patients, however, do not require these supplementary pain medications.
3. Headaches after the procedure (rare). Some patients can develop a minor headache after the procedure. It is not common.
4. Indentations in the area where the steroids were injected (atrophy). Indentations or depressions in the scalp can occur following injections but are much less common when low concentrations are used than when high concentrations are used. Indentations don’t occur in the first day or even in the first week. They develop over 2-4 weeks following the injections. Provided another set of injections is not performed into the area of scalp depressions (i.e. the atrophic area), the skin goes back to normal again in 2-4 months, and sometimes much sooner. If injections are performed into an area that is already atrophic, the recovery may take longer and in some cases be persistent (i.e. very long lasting or even forever).
5. Irregular periods (missed periods). Steroid injections performed in premenopausal and perimenopausal female patients can sometimes result in missed periods, irregular periods or changes in the length of the period or amount of bleeding. This too is not common but some women who receive many steroid injections for alopecia areata will note that their periods are irregular. some patents may even miss their period altogether - prompting some to wondering if they are pregnant or wondering if there is some issue for concern. Advising patients of this side effect before the steroid injections are performed can be very helpful.
Long term steroid injections: What do we need to counsel patients?
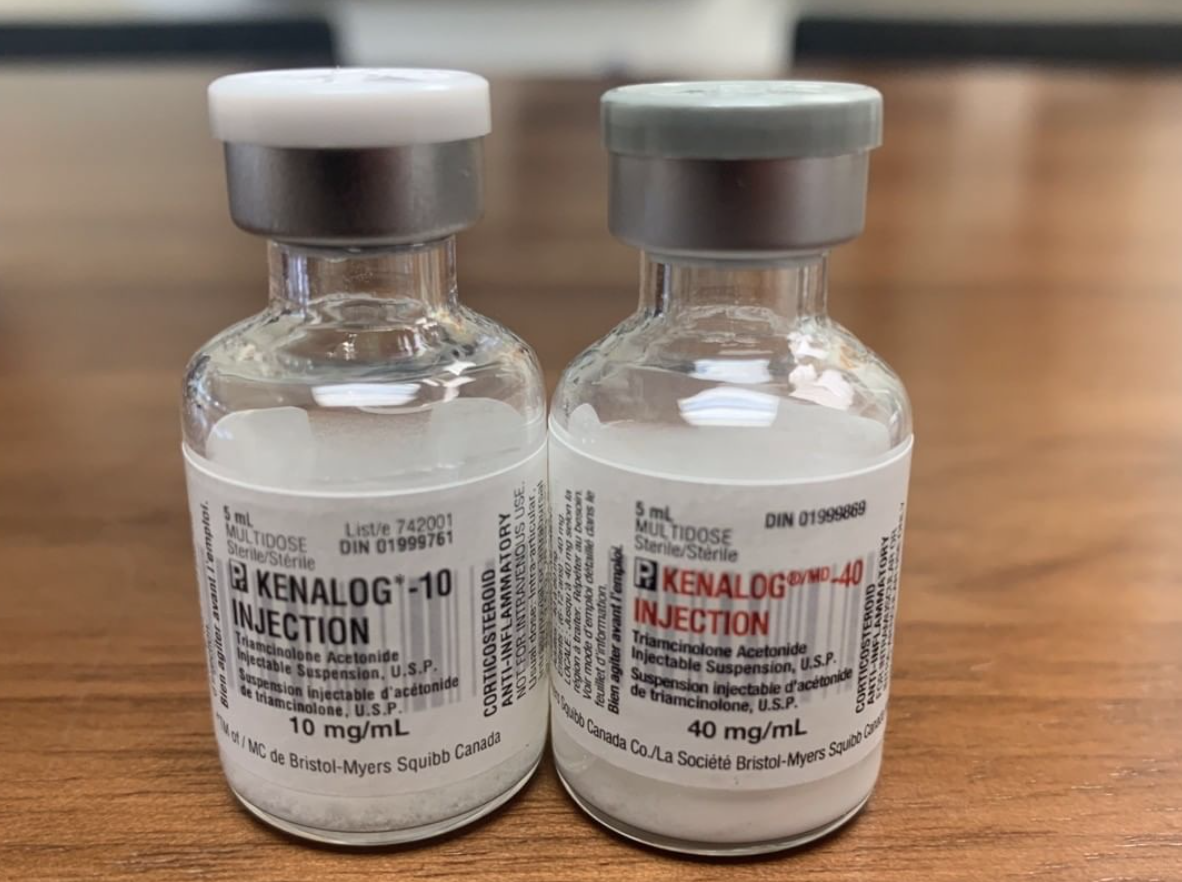
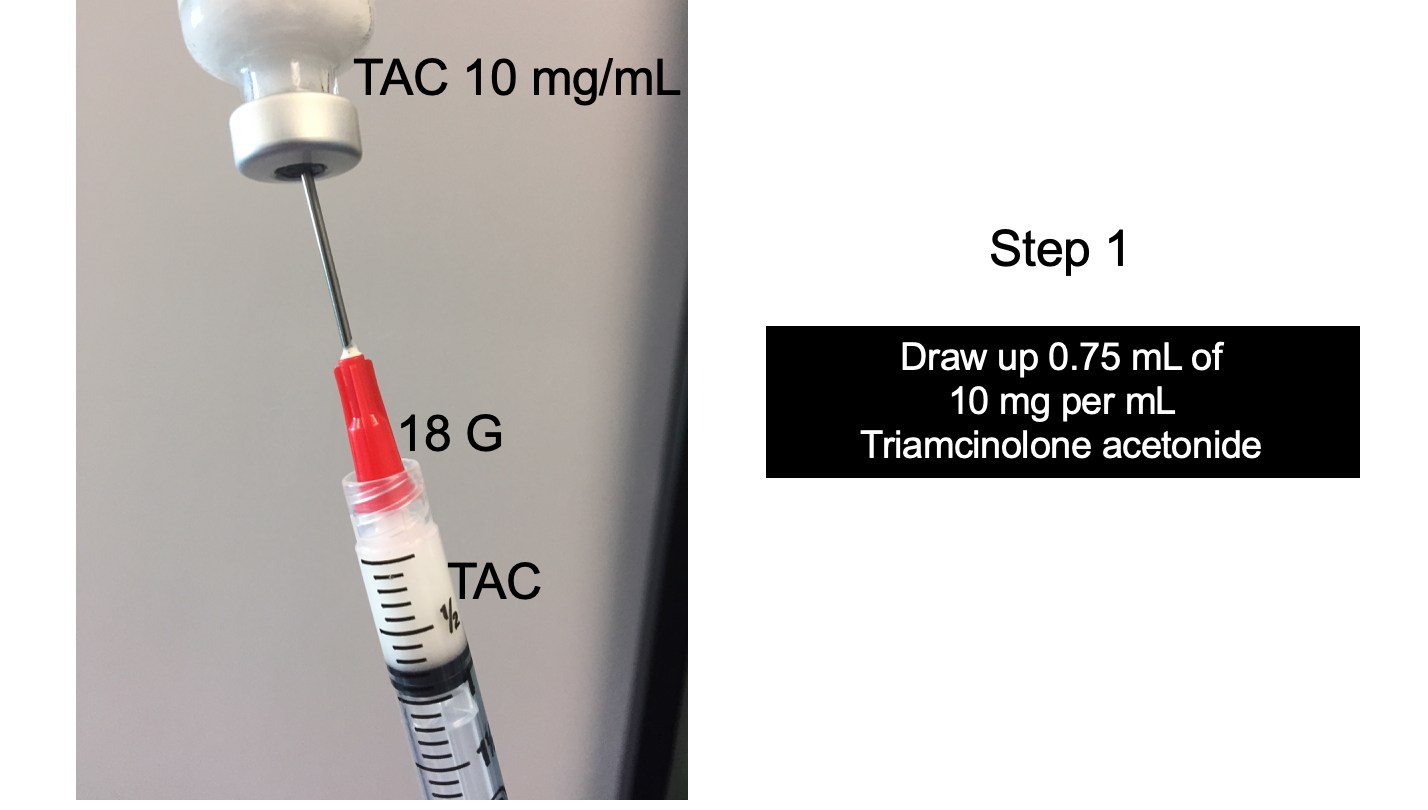
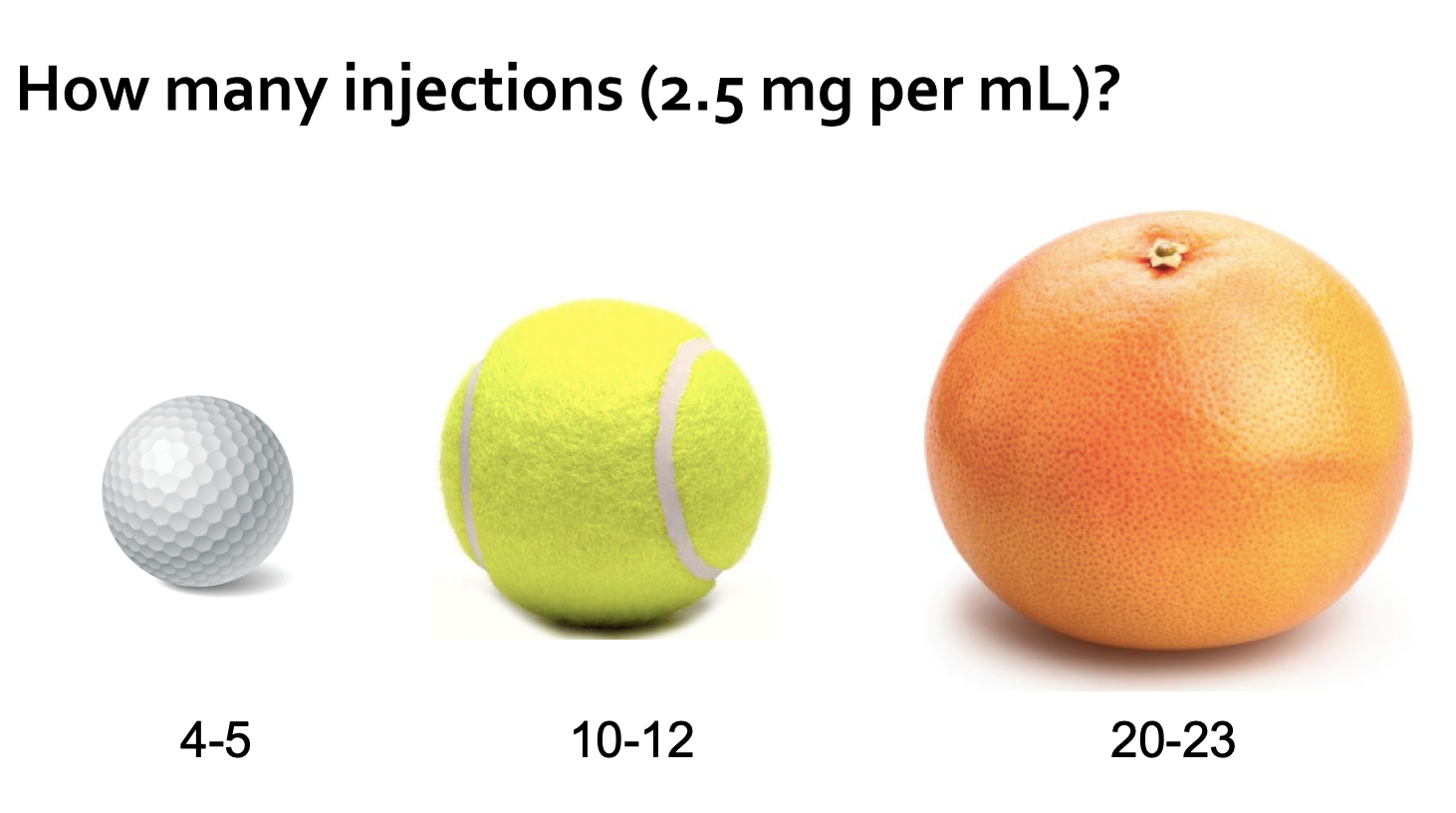
Steroid related side effects are still quite uncommon even in patients who receive many many steroid injections (i.e. such as monthly injections for 4-6 months). However, patients who are receiving steroid injections over the long term should be aware the steroid injections can be associated with a range of relatively uncommon side effects. These include acne, increased blood pressure, stretch marks (striae), bone thinning (osteopenia, osteoporosis), cataracts, blood sugar issues. and adrenal suppression and Cushing syndrome. Steroid injections in the eyebrow (i.e. for eyebrow alopecia areata) over many years may also increase the risk of cataracts. Side effects with long term steroid injections are still relatively uncommon - especially when the patient has many months of drug free holidays. The use of 2.5 mg per mL concentrations of triamcinolone acetonide (rather than 5 mg per mL of 10 mg per mL) may reduce absorption and therefore systemic side effects as well.
Setting up for steroid injections: What 9 supplies are needed?
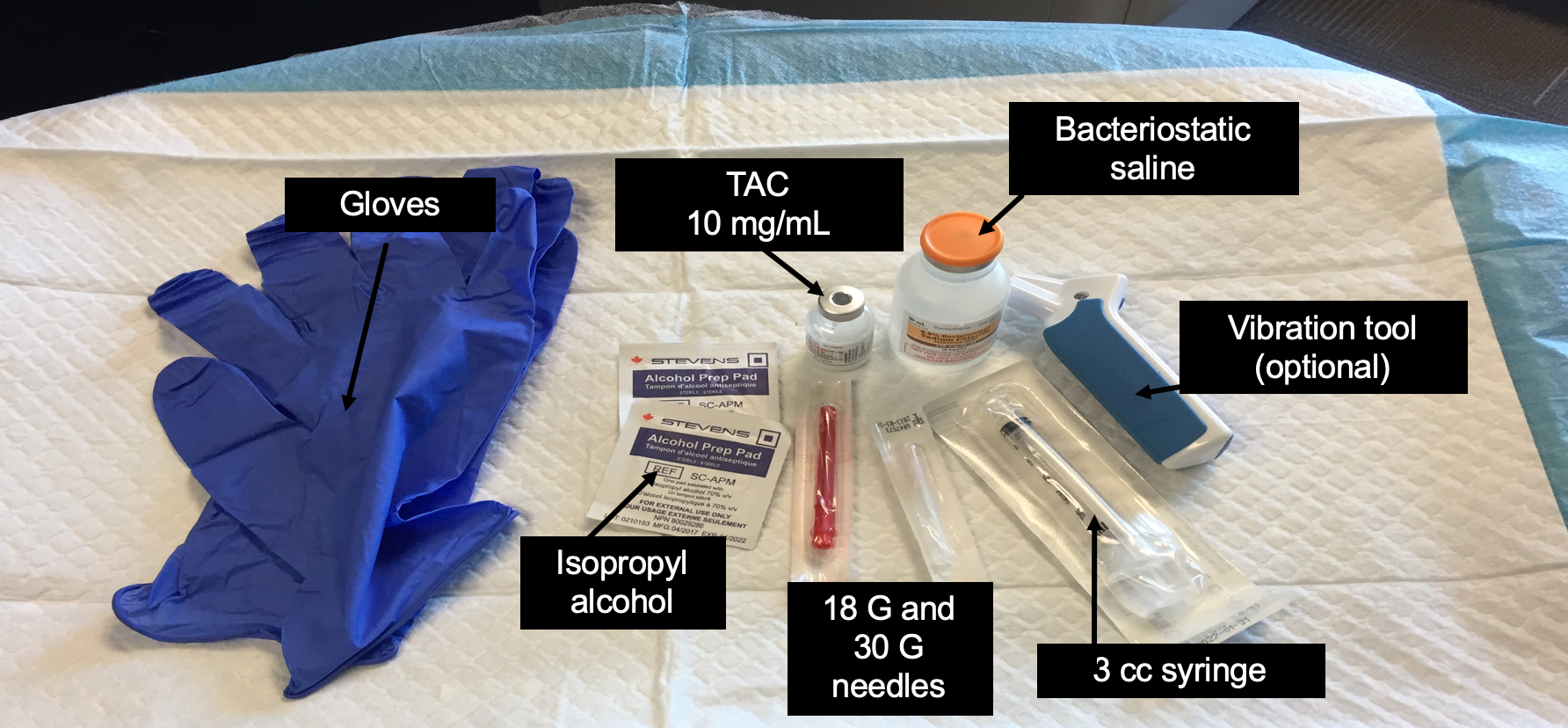
Steroid injections are easy to perform in the office setting and don’t require a great deal of supplies. The basic supplies are shown in the diagram below and include:
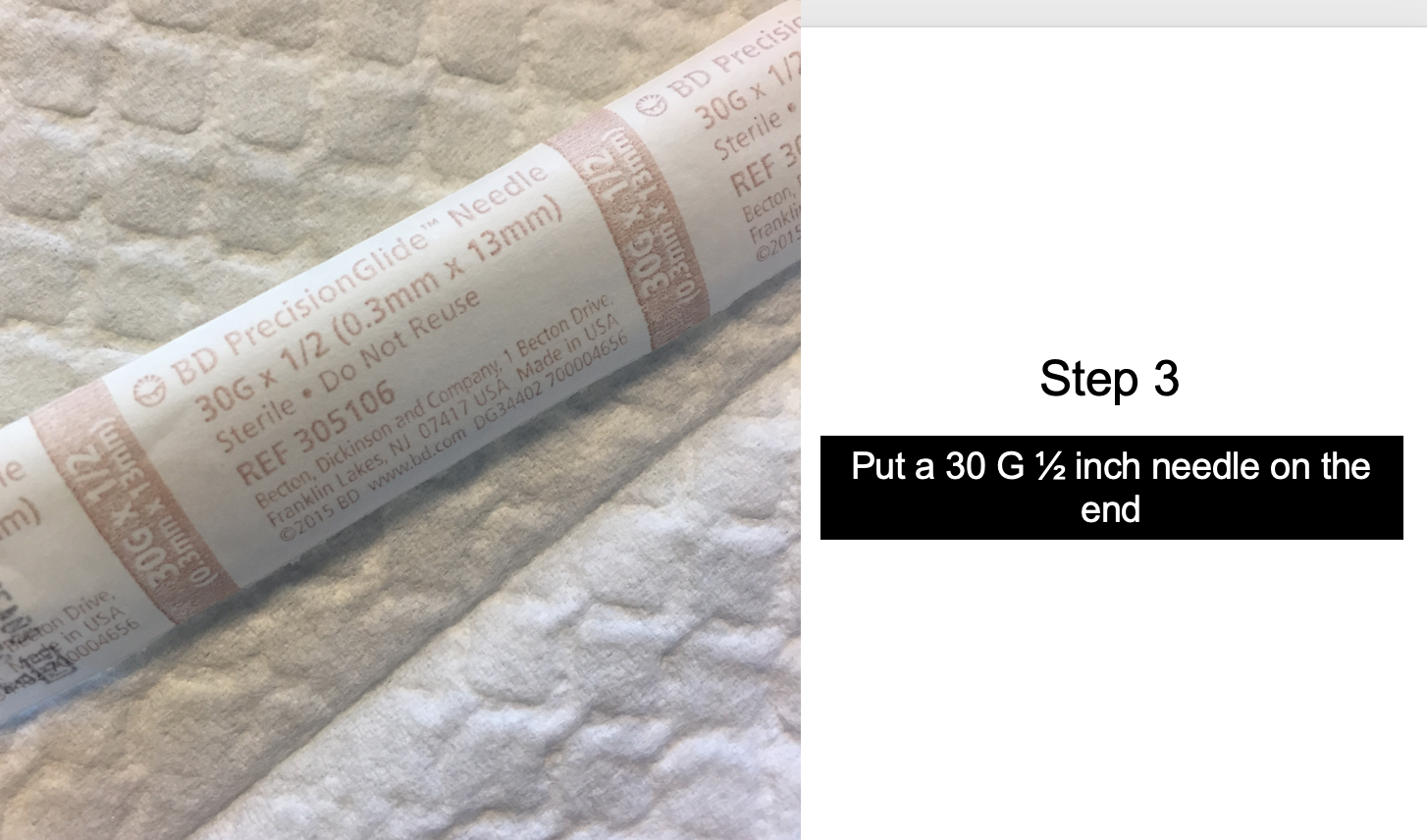
1) triamcinolone acetonide 10 mg per mL bottle 2) saline used for dilution 3) 3 mL syringes 4) alcohol swabs to wipe the top of the bottles of bacteriostatic injection grade saline and triamcinolone 5) 18 gauge needle to draw up the steroid and saline 6) 30 gauge needle to administer the triamcinolone into the scalp 7) vibration device to make the injections less painful and 8) gauze and 9) gloves.