What is the diagnosis? Trichotillomania vs Alopecia Areata
I’ve selected this question below for this week’s question of the week. It allows us to discuss some of the finer aspects of trichotillomania and alopecia areata - both of which are common diagnoses in children and teens. It can sometimes be tough to tell them apart as alopecia areata and trichotillomania both have broken hairs and black dots. Exclamation mark hairs can be found in both although one needs to be careful, in my opinion about using the term exclamation mark hair too liberally. In my opinion a true exaltation mark hair is quite a bit thinner at the bottom than it is at the top rather than “just a bit” thinner.
Here is the question….
Question
Hi! My daughter was diagnosed with alopecia areata two years ago... her first bald spot was right behind the ear...

Photo 1: Back of the scalp behind year in 2018. This is typical of alopecia areata
I took her to a dermatologist and she was given injections and the hair grew back.. soon after, the hair in the front of her head began to fall...

Photo 2: Front of the Scalp in 2020. As I will review below, features of trichotillomania are identified in this patch of hair loss. Alopecia areata can not be completely ruled out as a second diagnosis …. but features suggest trichotillomania without any doubt.
I questioned her numerous times about wether or not she was pulling the hair, but she always denied it... fast forward to the beginning of March... I took her to a dermatologist who was well versed on alopecia and she looked at her scalp thru a magnifying glass and said that she had alopecia and it was definitely AA... then with everything happening with COVID-19 we weren’t able to see see the specialist she recommended due to being on lockdown... this past week I had a heart to heart with my daughter and she admitted that she had in fact been pulling her hair out... so now I’m questioning the validity of the exclamation hair statement... I do see hair that looks like it could be so my question is can exclamation hair be present in someone suffering from Trichotillomania? Or is it only specific to alopecia? I appreciate any words of advice u can give... we have been so desperate these past two years doing anything and trying anything we could to make this stop... and now that she has admitted to pulling, maybe there’s light at the end of the tunnel... but maybe she also has alopecia... thanks again!
Answer
Thanks for submitting your question. This is a terrific one - and a challenging one too. However, I do feel that what we are seeing here is alopecia areata in the back fo the scalp (two years ago) and trichotillomania in the frontal region at the present time. I don’t see any good evidence for alopecia areata in the frontal region but it can’t be completely excluded. I just don’t feel that’s all that likely - at least as a major feature of the loss in this area.
The story is quite typical for your daughter having alopecia areata in 2018 at the back of the scalp. First, the appearance is quite typical of alopecia areata and the location is too, Second, the robust response to steroid injections is very much in keeping with alopecia areata as trichotillomania would not grow back quite so fast.
But let’s take a closer look at this region at the back of the scalp:

Photo 3: Magnified View of the Back of the Scalp Behind the Ears. This is typical of alopecia areata.
This is a pretty typical photo of alopecia areata. We see many broken hairs, black dots and vellus hairs. The other finding we see is what I term the “short long” sign. This is shown in the circle - one hair is long and a neighbour right next to it is short. This is very different than the “V sign” in trichotillomania where the fingers rip our hairs in a manner such that the hairs right next to each other are the same size:

V sign of trichotillomania compared to the short long sign of alopecia areata.
The Trichoscopic Features of Trichotillomania
So now that we are on the subject, what exactly are the trichoscopic features of trichotillomania. Well, they include broken hairs, v-sign, flame hairs, hair powder, tulip hairs, and coiled hairs among others. The most common are the irregularly broken hairs. The “v sign” represents two hairs that were pulled at the same time and snapped off at the surface. They are found in well over 50 % of patients with trichotillomania.
We’ve seen the V sign in the diagram above. Now let’s take a look at coiled hairs. Coiled and hook hairs represents hairs that recoil after being pulled out suddenly. They are found in well about one-third of patients with trichotillomania.

In fact, when we look up closer to the scalp, from the recent 2020 photos (from the frontal scalp), we see many features of trichotillomania including irregularly brown hairs, V hairs, hook hairs and tulip hairs and exclamation-mark like hairs.

Photo 4: Magnified view showing V sign

Photo 5: Magnified view showing “flame hair.”
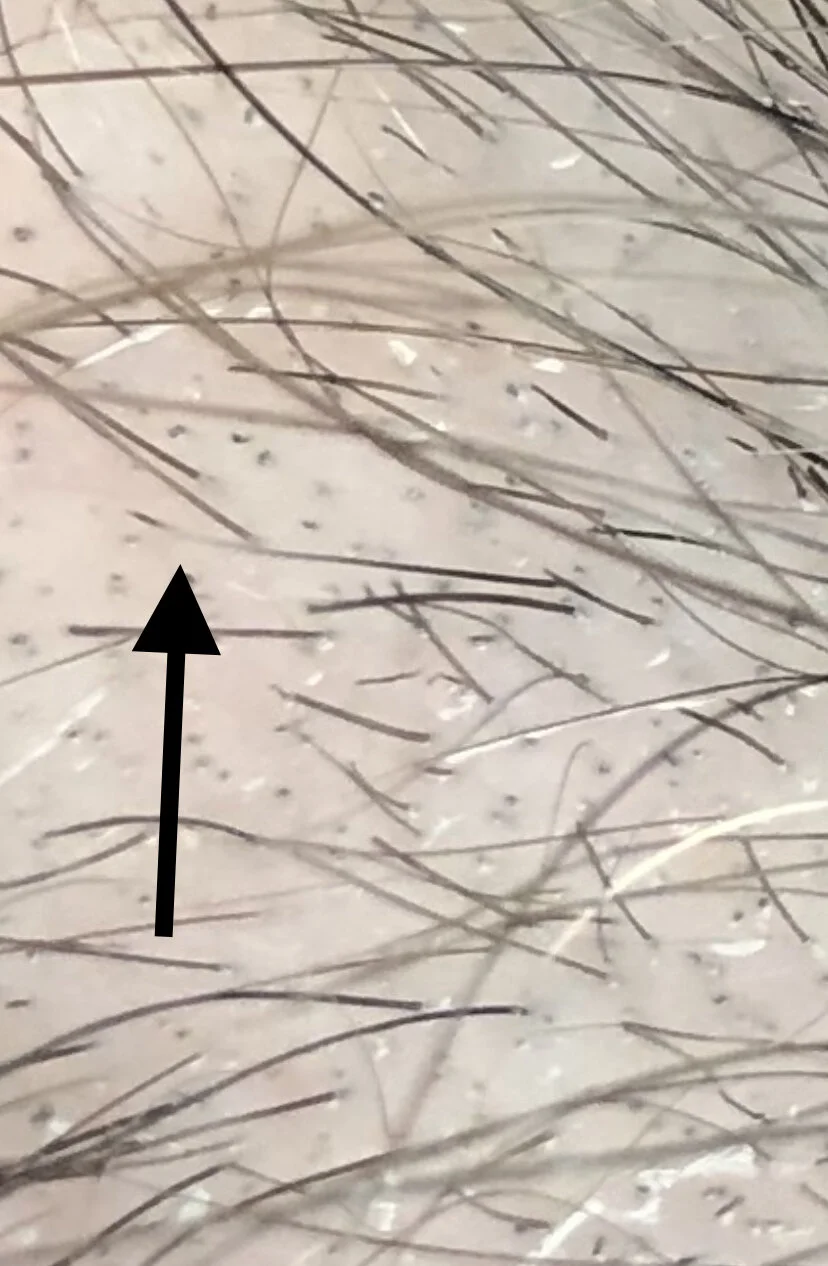
Photo 5: Magnified view showing “tulip hair.”

Photo 6: A pseudo exclamation mark hair. This hair is tapered but not tapered to the degree we expect in a classic exclamation mark hair. The hair is only slightly thinner at the bottom than the top. True exclamation mark hairs, in my opinion, are very thin as they enter into the scalp. They are less than 1/3 the thickness at the bottom compared to the hair at the top. This hair does not fit that definition so I term it a pseudo exclamation mark hair. Both true and pseudo exclamation mark hairs, can be seen in alopecia areata and trichotillomania although extremely tapered exclamation mark hairs are more common in alopecia areata.

Photo 7: Magnified view showing “hook hair.” Hook hairs are quite specific for trichotillomania.
Conclusion and Final Comments
Thanks for the submission to our Question of the Week Program. I hope this was helpful. In summary, the area at the back of the scalp back in 2018 is typical of alopecia areata and the area at the front of the scalp in 2020 is typical of trichotillomania. I can’t completely rule out “some” alopecia areata in the frontal scalp being present but it would not be the most likely scenario. A biopsy could ultimately prove whether there is any amount of alopecia areata in the front - but I don’t think this is necessary here. I know there may be a thought these are exclamation mark hairs but in my opinion they are not classic exclamation mark hairs but rather broken hairs and pseudo exclamation mark hairs. One can have exclamation mark hairs in alopecia areata and trichotillomania and this finding alone is not enough. We need to dig deeper. Here we have features of trichotillomania as the main features. It’s possible for both alopecia areata and trichotillomania to BOTH be present. It’s more likely to occur together in children younger than 5. In an older child and teen or adult, it’s more likely that trichotillomania alone or alopecia areata alone is the sole diagnosis in a case like this. But they can occur together, yes.
Your dermatologist can guide you further. One certainly needs to be humble that alopecia can always resurface in anyone who previously had the diagnosis. Ongoing surveillance is appropriate for anyone with a past diagnosis of alopecia areata. There is nothing wrong with speaking to the dermatologist about use of topical steroids or another steroid injection as there can be quite a bit of inflammation that also occurs in trichtotillomania. However, in this case, the regrowth of hair after injection does not mean the diagnosis was alopecia areata. Repeat photos fo the scalp and repeat trichoscopy can be helpful to monitor what is happening and whether in fact any amount of alopecia areata does appear again. A biopsy can be considered if there is any doubt or confusion but I’m generally against biopsies in situations like this because a) we can make the diagnosis without a biopsy and b) biopsies only add to the stress of the child or teen.
When the diagnosis of trichotillomania is made in children and teens, we need to pause and look carefully into the the child’s stressors. There can be underlying psychological and psychiatric issues present and the sooner these can be addressed the better for the child or teen. Not all children and teens with trichotillomania have underlying psychiatric issues but it’s far more likely to be present if the patient is a teenager than if they are preschoolers. A variety of issues such as depression and anxiety and eating disorders and obsessive compulsive disorders need to be explored. The dermatologist’s office may be a good place to start but the paediatric or general practitioner may be the next step and a psychologist or psychiatrist is sometimes needed if underlying psychiatric or psychological issues are present. Sometimes there are issues in the child’s life that a parent is fully aware. Sometimes there are issues that a a parent is only partly aware. And sometimes there are issues that a parent is not aware at all. I can’t emphasize enough how important this is to examine these sorts of issues more closely. If there are underlying issues, addressing them sooner can can change a child’s life forever for the better. The fact that the individual in this case has admitted to her parent that she pulls hair is a really important finding. It certainly speaks to better prognosis. A supportive rather than blame centred approach is what is needed next. It takes a lot of courage for a child or teen to admit pulling. Some individuals can stop easily and some can not. While I agree that there may be “light at the end of the tunnel” as you have said I would encourage you to be patient as this can be much more chronic than many parents first realize when the diagnosis is made. It all depends on the exact situation of course but the diagnosis is sometimes only step 1 in a long journey. Stopping the pulling may or may not relieve the underlying psychological issues. The long term measure of success here is not whether the hair grows back but whether the child or teen has been helped with whatever issues may have triggered the pulling in the first place.
Thank you again for participating in our question of the week program.
References of Interest
The “V sign” in Trichotillomania
Coiled Hairs and Hook Hairs in Trichotillomania
Trichotillomania: Addressing both scalp heath and emotional health